The new therapy aims to stimulate the brain with small currents applied to the scalp. Illustration by Harry Campbell
“What does this part of the brain do, again?” I asked, pointing to the electrode on my right temple.
“That’s the right inferior frontal cortex,” said Vince Clark, the director of the University of New Mexico Psychology Clinical Neuroscience Center, in Albuquerque. “It does a lot of things. It evaluates rules. People get thrown in jail when it’s impaired. It might help solve math problems. You can’t really isolate what it does. It has emotional components.”
It was early December, and night was falling, though it was barely five. The shadows were getting longer in the lab. My legs felt unusually calm. Something somewhere was buzzing. Outside the window, a tree stood black against the deepening sky.
“Verbal people tend to get really quiet,” Clark said softly. “That’s one effect we noticed. And it can do funny things with your perception of time.”
The device administering the current started to beep, and I saw that twenty minutes had passed. As the current returned to zero, I felt a slight burning under the electrodes—both the one on my right temple and another, on my left arm. Clark pressed some buttons, trying to get the beeping to stop. Finally, he popped out the battery, the nine-volt rectangular kind.
A Day in the Life of a Frequency Researcher
Maintenance of the body is more important that maintenance of your car. We are constantly bombarded with various pathogens, toxic chemicals, and allergens, particularly when traveling. Here is a typical day in the life of a frequency researcher.
Typical day of maintenance. Frequency subscribers have updates to these and thousands more frequencies.
Ebola Virus Frequencies Version 2.5
Ebola virus disease (EVD) or Ebola hemorrhagic fever (EHF) is the name for the human disease which may be caused by any of four of the five known ebola viruses. These four viruses are: Bundibugyo virus (BDBV), Ebola virus (EBOV), Sudan virus(SUDV), and Taï Forest virus (TAFV, formerly and more commonly Côte d’Ivoire Ebola virus (Ivory Coast Ebolavirus, CIEBOV)). EVD is a viral hemorrhagic fever (VHF), and is clinically nearly indistinguishable from Marburg virus disease (MVD).
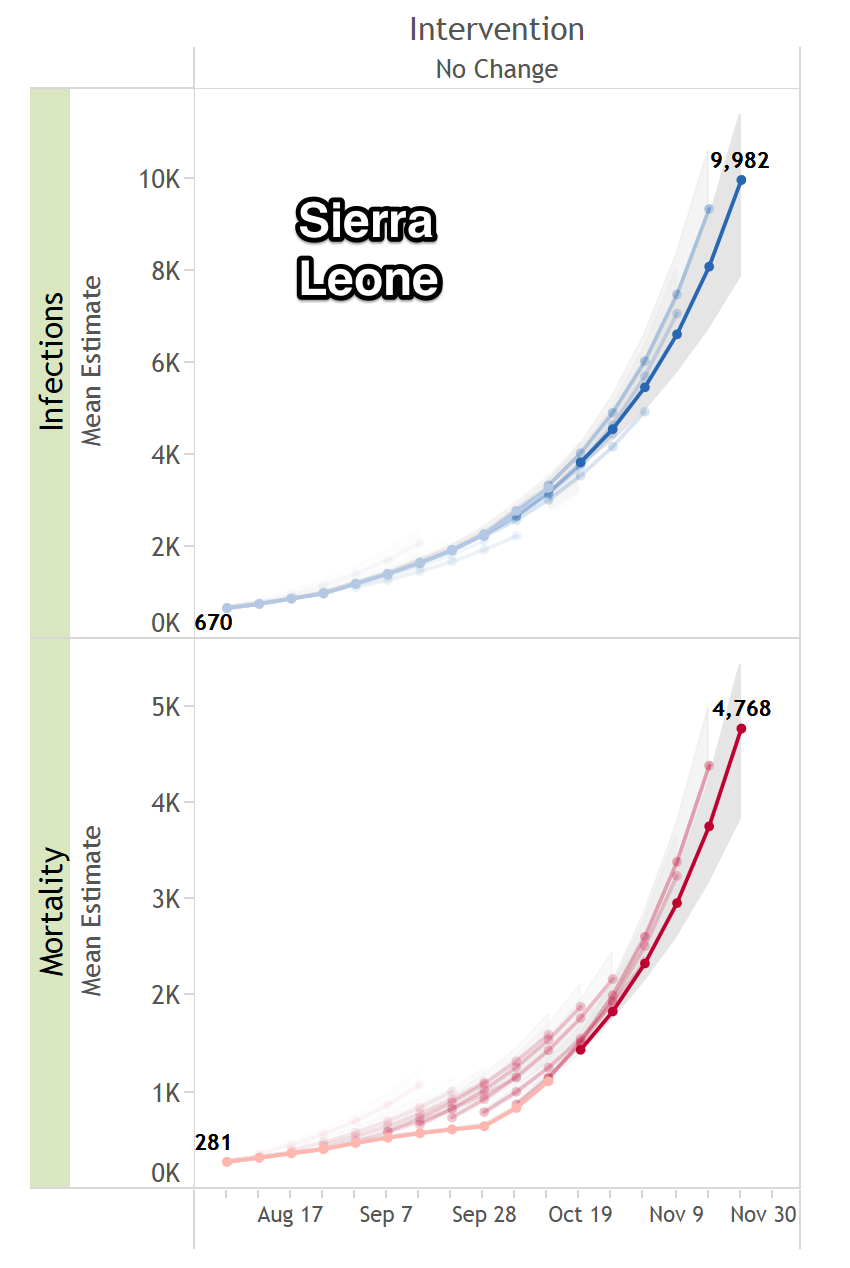
Dr. Keith Scott-Mumby writes, “Healthy well-fed victims of Ebola who died: zero. Undernourished, already-sick victims of Ebola who died: 2,461 to date. Serious fatality: the truth. Note that the rough figures released last week put total cases at around 6,500 and deaths at 2,200, that means it’s only about 30% fatal and NOT 90% as the US media keep screaming in their scare frenzy. Four healthy, well-fed Americans have contracted Ebola and survived comfortably. As I told you a couple of weeks ago, the supposed savage image of this infection had more to do with the terrain it’s in, meaning among peoples who are shocked, overloaded with toxins, under-nourished and weary from decades of internecine wars. But the manufacture of hysteria continues.”
The new Frequency Research Foundation update available to frequency subscribers includes new ebola virus strains, including a virulent strain seen in Africa, as well as updates to previously published frequencies. Several U.S. infections have been eliminated with these frequencies and a clear pattern has emerged in Hadoscan runs for those with more serious infections.
This frequency set is now being transmitted by parasites like the flu. Mild cases will be asymptomatic or cause general malaise for about a week. More serious cases will put you in bed.
A while back a subscriber asked me to pull together ebola virus frequencies, all of which were embedded in the lyme frequencies. The good news for lyme sufferers is that you have some immunity to almost all the nasty viruses in the world including several strains of ebola virus. The bad news is that if you don’t eliminate them with frequencies they will be circulating in your system for a lifetime.
The ebola viruses sometimes travel with the swine flu which is also a lyme based disease. At least one ebola strain can cause your skin to slough off it you get a bad infection, so it is good to have these frequencies in your emergency toolkit.
Even in the worst case it takes a while to die of the ebola virus and that is long enough to eliminate it with frequencies. What can make it challenging is if the route of infection is a parasite (as is commonly the case). Then you must kill the parasites or they keep reinfecting you (the reason flu is so hard to eliminate). There are two parasite sequences in the current ebola set known to be associated with the ebola virus. There may be more.
Also, viruses come in groups of at least two or three, as a single virus cannot usually overwhelm the immune system. A recent case of ebola infection was associated with rhabdovirus carpia, another virus seen commonly in lyme disease and swine flu infections.
To obtain frequencies become a subscriber using the link on the right side of the page.
Candida: Everybody Has It But How To Get Rid of It!
Use Aqua Flora in combination with frequencies to eliminate candida.
Candida is pandemic – almost everyone has a candida infection. These infections have been stimulated by overuse of antibiotics and the problem gets worse as time goes on. Recently, fungal infections including candida have been tied to cancer, so this is not an innocuous infection.
Even if you avoid antibiotics you can get infected with candida. Flu infections are transmitted by parasites which contain multiple strains of flu virus, bacteria, other pathogens, and often candida. The candida fungus can get on clothes and other materials where you can pick up a contact infection. Loving your partner can give you a candida infection.
Over half the population is infected with Lyme organisms (at least over half of the people I test) and the Lyme complex includes many strains of candida along with many other organisms.
Candida is extremely persistent and thrives on diets rich in sugar. Most physicians will advise altering diet yet this is only a stopgap measure. It doesn’t eliminate candida, it just slows down its growth. Candida pairs up with sets of other organisms and toxic compounds to cause disease syndromes as it is a good immune suppressant allowing other pathogens to proliferate.
The only way I have found to completely eliminate candida is to target each strain with frequencies. This is a complex problem as there are many strains and each strain has multiple forms that require multiple frequencies.
It is not possible to eliminate these strains unless you target all the forms of the organism. It has taken over a decade of research to enable easy identification of these frequency sets so and Frequency Research Foundation subscribers have access to dozens of frequency sets for candida strains.
Aqua Flora should be taken while working on candida frequencies. It is a harmless, yet potent, homeopathic remedy. A teaspoon in a glass of water is best. Drink a tablespoon of this water several times a day and rub the water on affected areas. This alone will eliminate most symptoms.
Swine Flu 2014 Frequency Sets Released
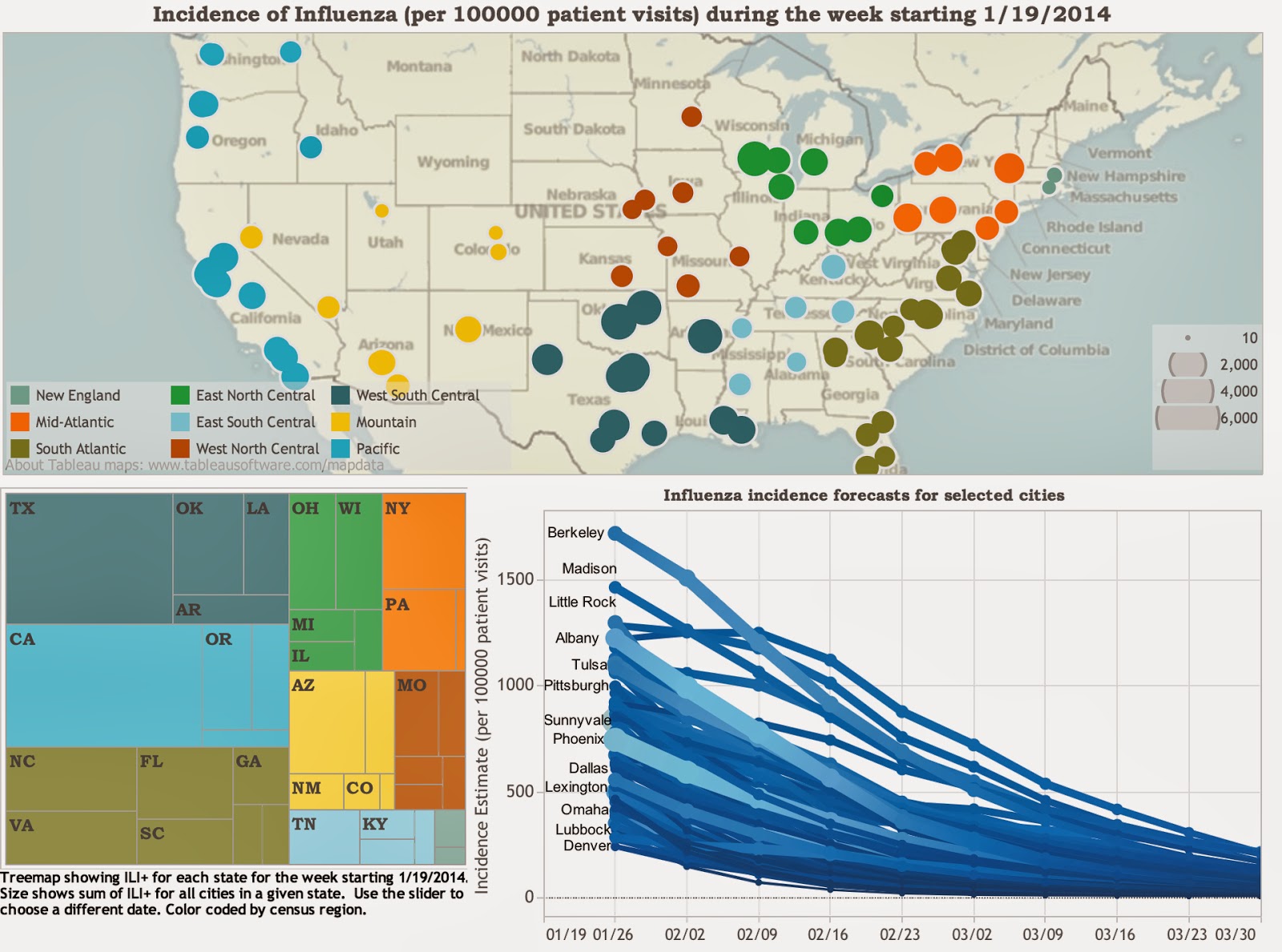
Flu Predictor The flu season has peaked and this season has several new strains of swine and avian flu along with some biofilms that are giving people staph infections. As usual, the flu is communicated by airborn parasites.
A new Flu Predictor has been developed at Columbia University which is useful for seeing the trend of flu infections in your area. See Flu Predictor news.
Most people also have residual infections from Swine Flu 2013. Frequency research this year has added many biofilms to the flu sets.
All of these frequency sets are available to Frequency Foundation subscribers.
Shattering Cancer Cells with Frequencies (technology is decades old)
This is decades old news but useful information for the uneducated. It shows how to kill cancer cells and other organisms with frequency devices. Dr. Bare did not invent this technology as it was invented by Royal Rife in the 1920’s.
Frequency Surgery: Star Trek Technology in Israel
For all you pseudoscientists out there who don’t believe frequencies are the future of medicine, take a look at the latest surgery technique in Israel, totally based on sound frequencies.
About 10 years ago, at the MIT Future of Health Technology annual conference I demonstrated the use of the FSCAN to identify frequencies for pathogens and then use the same frequencies for eliminating the pathogens. I was moved to do this after a COMPAQ presentation of an ultrasound device that scanned the patient and then used ultrasound frequencies to heal the patient. This was the first commercial product that is the forerunner of Star Trek Tricorder technology. You scan and heal the patient with the same frequency device.
It is easier to bring sound frequencies into the operating room because ultrasound has gone through decades of clinical trials. Electromagnetic frequencies are in earlier stages and can be see in Bill Doyle’s Ted Talk on treating brain cancer with EMF in FDA clinical trials.
EM Patent by Elizabeth Rauscher
United States Patent
4,889,526
Rauscher , et al.
December 26, 1989
Non-invasive method and apparatus for modulating brain signals through an external magnetic or electric field to reduce pain
Abstract
This invention incorporates the discovery of new principles which utilize magnetic and electric fields generated by time varying square wave currents of precise repetition, width, shape and magnitude to move through coils and cutaneously applied conductive electrodes in order to stimulate the nervous system and reduce pain in humans. Timer means, adjustment means, and means to deliver current to the coils and conductive electrodes are described, as well as a theoretical model of the process. The invention incorporates the concept of two cyclic expanding an collapsing magnetic fields which generate precise wave forms in conjunction with each other to create a beat frequency which in turn causes the ion flow in the nervous system of the human body to be efficiency moved along the nerve path where the locus of the pain exists to thereby reduce the pain. The wave forms are create either in one or more coils, one or more pairs of electrodes, or a combination of the two.
Inventors:
Rauscher; Elizabeth A. (San Leandro, CA), Van Bise; William L. (San Leandro, CA)
Assignee:
Magtech Laboratories, Inc. (Reno, NV)
Appl. No.:
07/120,914
Filed:
November 13, 1987 Contact Dr. Donnie Rudd for a new low cost magnetic healing device based on this patent.
Shingles Frequencies Version 2.0: You Will Need Them As You Age!
from Wikipedia
Herpes zoster (or simply zoster), commonly known as shingles and also known as zona, is a viral disease characterized by a painful skin rash with blisters in a limited area on one side of the body, often in a stripe. The initial infection withvaricella zoster virus (VZV) causes the acute (short-lived) illness chickenpox which generally occurs in children and young people. Once an episode of chickenpox has resolved, the virus is not eliminated from the body but can go on to cause shingles—an illness with very different symptoms—often many years after the initial infection. Herpes zoster is not the same disease as herpes simplex despite the name similarity (both the varicella zoster virus and herpes simplex virus belong to the same viral subfamily Alphaherpesvirinae).
Varicella zoster virus can become latent in the nerve cell bodies and less frequently in non neuronal satellite cells of dorsal root, cranial nerve or autonomicganglion,[1] without causing any symptoms.[2] Years or decades after a chickenpox infection, the virus may break out of nerve cell bodies and travel down nerve axons to cause viral infection of the skin in the region of the nerve. The virus may spread from one or more ganglia along nerves of an affected segment and infect the corresponding dermatome (an area of skin supplied by one spinal nerve) causing a painful rash.[3][4] Although the rash usually heals within two to four weeks, some sufferers experience residual nerve pain for months or years, a condition called postherpetic neuralgia. Exactly how the virus remains latent in the body, and subsequently re-activates is not understood.[1]
Throughout the world the incidence rate of herpes zoster every year ranges from 1.2 to 3.4 cases per 1,000 healthy individuals, increasing to 3.9–11.8 per year per 1,000 individuals among those older than 65 years.[5][6][7] Over a lifetime, a large fraction of people develop herpes zoster, though usually only once – in a 1960s US study, 50% of individuals living to age 85 had at least one attack, while 1% had at least two attacks.[8]Antiviral drug treatment can reduce the severity and duration of herpes zoster if a seven-to-ten day course of these drugs is started within 72 hours of the appearance of the characteristic rash.[5][9]
A recent full blown case of shingles (hospital diagnosed) in a client allowed identification of many strains of the shingles virus. The rash was stopped from spreading immediately with frequencies and the client was puzzled as to why she had such a mild cash of shingles after going to the hospital emergency room prior to frequency application.
Upon further investigation, the client slept in a houseboat in Amsterdam that had mosquitos infected with the shingles virus. A mosquito bite on the leg started the shingles rash. Because she had latent shingles virus from smallpox in childhood, she developed a full blown infection. The houseboat was cleared of mosquitos using the Frequency Foundation Mosquito Service and cleared of the shingles virus with the shingles frequencies. It turns out that there are many strains of the shingles virus that must be eliminated!
The Life Extension Foundation reported the following in December 2012:
Following a chicken pox infection, the virus (called varicella-zoster, or VZV) takes refuge in nerve cells. With the onset of immunosenescence, it’s only a matter of time until the virus can reemerge to trigger an attack of shingles. Here are some surprising fiures about this classic illustration of immunosenescence at work.
More than 90% of adults harbor the VZ virus, and there is no means of predicting when or in whom a shingles outbreak will occur.
It’s estimated that 1 million new cases of shingles occur in the US each year, resulting in up to 60,000 hospitalizations.
Your risk of developing shingles is about 1 in 3.
With advancing age, your risk of developing shingles goes up dramatically: by age 85, 50% of people have had at least one outbreak.
The severity of a shingles outbreak increases with age.
As a result over 90% of adults will benefit from running shingles frequencies to clear the virus from their body. Additional strategies for reversing immunosenescence are also recommended.
Frequencies are available with a subscription to the Frequency Foundation.
Tuberculosis Frequencies Version 3.0
An Armenian doctor showing chest x-rays used to track a patient’s tuberculosis that has been resistant to drug therapy. By NICHOLAS D. KRISTOF Published: New York Times, December 6, 2008
Update 11 Nov 2012: Tuberculosis frequencies have been repeatedly updated since 2008 and Version 3.0 is available. Certain strains of the swine flu included tuberculosis. In the opinion of this researcher, most deaths due to swine flu were caused by the swine flu viruses, bacteria, and parasites combined with tuberculosis. In addition, more virulent strains of tuberculosis have appeared, even more resistent to antibiotics than XDR tuberculosis.
This means that those interested in the latest tuberculosis frequencies should subscribe to the Frequency Foundation list where all updates are posted. See this link …
All frequencies are based on original research on thousands of people, animals, microscopic slides, and high-resolution digital photos and microscopic images of the actual organisms. The Frequency Foundation database contains many gigabytes of original raw frequency data from a decade of research and these data are researched and refined to continually update frequency sets. For questions, errors, or omissions contact: [email protected]. Frequencies are for research purposes only and may be helpful, harmful, or ineffective depending on how they are used. These programs may generate negative side effects in the form of Herxheimer reactions or other phenomenon and are only to be used by other researchers for experimentation at their own risk.
Upgrade to Version 2.2
Ongoing research added another strain of XDB-TB and parasites associated with this organism.
Upgrade to Version 2.0
The New York Times recently provided new photos on a case of drug resistant tuberculosis that are useful for enhancing the tuberculosis frequency set. Many cases have been examined by the Frequency Foundation through electronic media and all cases have the same virus associated with the tuberculosis organism. This virus has been added to the frequency set. It appears that a number of persistent bacteria harbor a virus that helps protect them by reducing immune function and, in this case, reducing respiratory function. Fortunately, it is remarkably easy to eliminate this complex of organisms with frequencies.
From the point of view of frequency research, XDR-TB, MDR-TB, and TB are very different organisms. Each is included in the attached frequency set. There may be additional strains and there may be other helper viruses. That is a topic for future research when modifications are needed to eliminate new strains of the organisms.
In the 1980’s, after spending many years as a professor at the University of Colorado School of Medicine, it was clear that drug technology is a 1940’s technology that will not take us into the future. Suppression of innovation in medicine by business interests has assured that we will not have the technology of the future until enough people die unnecessarily that people start demanding something different. For example, I recently suggested to a physician at one of the world’s largest non-profit organizations trying to eradicate tuberculosis and malaria that they try some frequency work. I was told if they experimented with frequency devices they would lose all their grants. Innovation is being systematically suppressed by your government and your physicians are living in fear of losing their livelihoods.
Imagine if IBM has been able to suppress chip innovation. We would have to build a laptop with vacuum tubes and use a truck to haul it around. This is the situation we are in with drugs. Innovation in electronics can completely replace drugs. The healing tool of the future will be our laptop or smartphone. It will have a database for frequency transmission that can emulate any drug. Frequency Foundation is already using technologies that detect and prevent disease before you even know you have it.
It would be an excellent idea to experiment with and gain an understanding of how to use the tuberculosis frequencies with the many Rife technologies widely available on the market. Because about 1/3 of the population has latent infections with tuberculosis organisms, you may need to eliminate a ticking time bomb that can erupt when your immune system is suppressed for any reason.
It will take a worldwide grass roots movement to eliminate XDR:TB so I am releasing the frequencies under a Creative Commons License that allows anyone to use them for non-commercial purposes with attribution.
The frequencies are in F100 programming language format. This is thoroughly documented at atelierrobin.net.
Ongoing research will update these frequencies. For documentation of these frequencies and to obtain updates to these and many other frequency sets you can subscribe to the Frequency Foundation by clicking on the button below. Be advised that these frequencies will be upgraded as organisms mutate based on ongoing research and only subscribers will receive updates.
Manage Cookie Consent
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.