The Discovery: Herpes Virus DNA Found Inside Alzheimer’s Plaques
In 2009, a research team led by Dr. Ruth Itzhaki at the University of Manchester published a finding that should have changed the course of Alzheimer’s research. Using advanced molecular techniques, they examined brain tissue from Alzheimer’s patients and made a striking discovery: herpes simplex virus type 1 (HSV-1) DNA was found directly inside amyloid plaques — the hallmark pathological feature of Alzheimer’s disease.
The numbers were remarkable. In Alzheimer’s disease brains, 90% of amyloid plaques contained HSV-1 DNA. And 72% of all HSV-1 DNA found in these brains was located within the plaques themselves. The virus was not merely present in the brain alongside the plaques. It was embedded within them.
We published this article in 2010 because the implications were too significant to overlook. If a common virus was directly contributing to the formation of Alzheimer’s plaques, it meant that the disease might be preventable — and treatable — through antiviral approaches, including frequency-based protocols.
What the Study Found
The research, published in the Journal of Pathology (2009, Vol. 217, Issue 1, pages 131-138), was conducted by Wozniak, Mee, and Itzhaki at the Faculty of Life Sciences, University of Manchester.
The Method
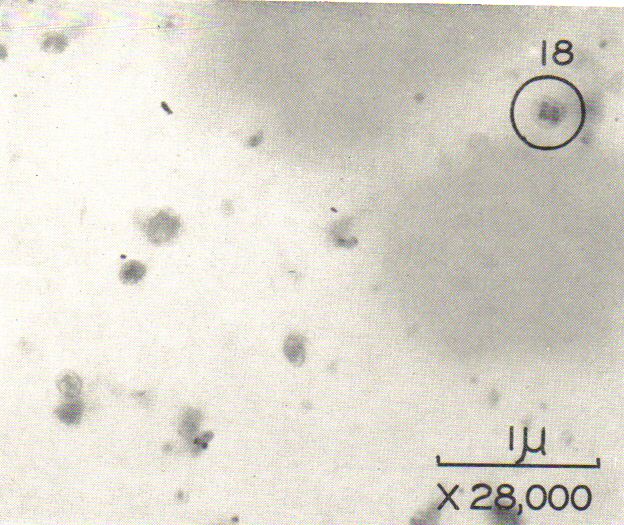
The researchers used a technique called in situ polymerase chain reaction (PCR) to detect HSV-1 DNA directly within brain tissue sections. They combined this with immunohistochemistry and thioflavin S staining to identify and visualize amyloid plaques. This dual approach allowed them to see exactly where the viral DNA was located relative to the plaques — not just whether both were present in the same brain, but whether they occupied the same physical space.
The Key Findings
The results were consistent across multiple brains and showed a clear pattern.
In Alzheimer’s disease brains, 90% of amyloid plaques contained herpes simplex virus type 1 DNA. Additionally, 72% of all viral DNA detected was physically associated with plaque deposits.
In aged normal brains — which also develop some amyloid plaques, though at a lower frequency — 80% of plaques still contained HSV-1 DNA. However, only 24% of the total viral DNA was plaque-associated. This difference was statistically significant (p < 0.001).
The researchers interpreted this difference as evidence that healthy aging brains are better at clearing amyloid beta (Aβ), so less of the viral DNA ends up trapped within plaque deposits. In Alzheimer’s brains, the accumulation and impaired clearance of amyloid means more viral DNA becomes permanently embedded in the growing plaques.
What This Means
The study’s authors stated their conclusion directly: HSV-1 “is a major cause of amyloid plaques and hence probably a significant aetiological factor in Alzheimer’s disease.” They recommended pursuing antiviral agents as treatment and potentially vaccination as prevention.
This was a bold conclusion in 2009. The Alzheimer’s research establishment was heavily invested in the “amyloid hypothesis” — the idea that amyloid plaques are the primary cause of the disease and that removing them should cure it. The suggestion that a virus was driving plaque formation challenged this framework at its foundation.
Why This Was Ignored — And Why It Matters Now
Despite the strength of Itzhaki’s findings, the infectious theory of Alzheimer’s was largely sidelined by the mainstream research community for years. Billions of dollars continued to flow into amyloid-targeting drug development, most of which failed in clinical trials. Meanwhile, the evidence connecting HSV-1 to Alzheimer’s continued to accumulate quietly.
The Frequency Research Foundation recognized the significance of this research immediately. When we published this article in 2010, the herpes-Alzheimer’s connection was considered fringe. Today, it is one of the most actively investigated areas in Alzheimer’s science.
2025 Update: 15 Years of Validation
Since the Wozniak, Mee, and Itzhaki study, the evidence linking herpes simplex virus to Alzheimer’s disease has grown from a single provocative finding into a substantial body of research involving millions of patients.
Large Population Studies Confirm the Link
Multiple large-scale epidemiological studies have now demonstrated that people with HSV-1 infections have a significantly higher risk of developing Alzheimer’s disease. Crucially, several of these studies have shown that antiviral treatment reduces that risk. A landmark 2018 study from Taiwan involving over 33,000 subjects found that individuals treated with anti-herpes medications had a dramatically lower incidence of dementia compared to untreated HSV carriers. This was the type of evidence that moves a theory from “interesting” to “actionable.”
The Mechanism Is Now Well Understood
Research since 2009 has clarified how HSV-1 drives Alzheimer’s pathology. The current understanding involves a cyclical process. HSV-1 resides dormantly in nerve tissue, including the trigeminal ganglion near the brain. When the virus reactivates — which can happen repeatedly throughout life due to stress, immune suppression, or aging — it travels to the brain and causes direct neuronal damage. The brain’s immune response to viral reactivation includes the production of amyloid beta, which has antimicrobial properties. Amyloid beta effectively traps the virus but accumulates over repeated cycles of reactivation, eventually forming the characteristic plaques of Alzheimer’s disease. Each cycle of viral reactivation triggers neuroinflammation, compounding the damage.
This means amyloid plaques may not be the cause of Alzheimer’s — they may be the brain’s defensive response to a chronic viral infection. This reframing explains why drugs designed solely to remove amyloid plaques have largely failed: they address the symptom, not the cause.
The APOE-ε4 Connection
Itzhaki’s earlier research had shown that HSV-1 is a particularly strong risk factor for Alzheimer’s in people who carry the APOE-ε4 gene variant — the best-known genetic risk factor for the disease. Subsequent research has confirmed this interaction. The APOE-ε4 allele appears to impair the brain’s ability to control HSV-1 reactivation, leading to more frequent viral flare-ups and faster plaque accumulation. This explains why some people with HSV-1 develop Alzheimer’s while others do not — the combination of the virus and the genetic variant creates the highest risk.
The Antimicrobial Hypothesis Gains Mainstream Support
What was once called the “herpes hypothesis” has evolved into the broader “antimicrobial protection hypothesis” of Alzheimer’s disease, championed by researchers at Harvard and other major institutions. This framework recognizes that amyloid beta functions as an antimicrobial peptide — part of the brain’s innate immune system — that responds to pathogens including HSV-1, bacteria, and fungi. Alzheimer’s, in this view, is the result of chronic, repeated immune activation in the brain.
The Connection to Other Chronic Infections
HSV-1 is not the only infectious agent linked to Alzheimer’s. The broader pattern is that chronic, brain-infiltrating infections drive the neuroinflammatory cycle that produces Alzheimer’s pathology. At the Frequency Research Foundation, we have been tracking these connections across multiple pathogen types.
Mycoplasma infections can cross the blood-brain barrier and contribute to ongoing neuroinflammation. Our research on mycoplasma is documented in Mycoplasma: A Key Component in Lyme and Other Diseases and Mycoplasma – Why the Lyme Flu Goes On and On.
Lyme disease spirochetes can directly invade brain tissue and trigger immune responses similar to those caused by HSV-1. Our Lyme disease frequency protocols address this neurological component.
The common thread across all these infections is chronic neuroinflammation. Managing this inflammatory burden is critical to slowing or preventing Alzheimer’s progression. Our article Eliminating Inflammation Is a Top Priority for Disease Prevention explains why this is the foundational strategy.
How Frequency Therapy Addresses the HSV-1 Connection
This research has direct and practical implications for frequency therapy. If HSV-1 is a significant driver of Alzheimer’s pathology, then addressing the virus with targeted frequencies — rather than waiting for plaque formation and trying to clear plaques after the fact — represents a fundamentally different treatment strategy.
At the Frequency Research Foundation, Dr. Jeff Sutherland has developed frequency protocols that target multiple aspects of the HSV-1/Alzheimer’s connection. Antiviral frequencies target HSV-1 directly, potentially reducing the frequency and severity of viral reactivation episodes in the brain. Anti-inflammatory frequencies address the neuroinflammation triggered by each reactivation cycle. Gamma frequency restoration, particularly 40 Hz stimulation, supports the brain’s natural clearance mechanisms for amyloid beta. Immune support frequencies help the body maintain better viral suppression over time.
This multi-layered approach addresses the cause (the virus), the mechanism (neuroinflammation), and the consequence (amyloid accumulation and cognitive decline) simultaneously. It is the type of comprehensive strategy that the research now supports.
Our flagship protocol, Alzheimer’s Disease – Version 2.0, incorporates antiviral frequency components alongside gamma stimulation and neuroinflammatory targeting. For the complete picture of how frequency therapy addresses Alzheimer’s from every angle, read our complete guide to Alzheimer’s disease and frequency therapy.
If you or a loved one is dealing with Alzheimer’s or cognitive decline, a consultation with Dr. Jeff Sutherland can assess whether chronic viral infections may be a contributing factor and develop a personalized frequency protocol to address it. Book Your Consultation
Frequently Asked Questions
Take the Next Step
The herpes-Alzheimer’s connection is no longer a fringe theory — it is supported by 15 years of research involving millions of patients. If chronic viral infection is driving Alzheimer’s pathology, then addressing that infection early and comprehensively is one of the most important steps you can take.
Dr. Jeff Sutherland has spent decades developing frequency protocols that target the infections, inflammation, and brain wave disruptions that contribute to Alzheimer’s disease. A paid consultation is the most direct way to explore what frequency therapy can offer for your specific situation.
Book Your Consultation with Dr. Jeff Sutherland
This article is part of our comprehensive Alzheimer’s resource library. Herpes simplex virus is one of several chronic infections linked to Alzheimer’s disease. Read our complete guide to Alzheimer’s disease and frequency therapy for the full scope of research, from 40 Hz gamma science to nutritional strategies and personalized frequency protocols.
© Frequency Research Foundation. This content is for educational and informational purposes only. It is not intended to diagnose, treat, cure, or prevent any disease. Always consult with qualified healthcare professionals regarding medical conditions.